Get Cna Shower Sheets Form in PDF
Get Cna Shower Sheets Form in PDF
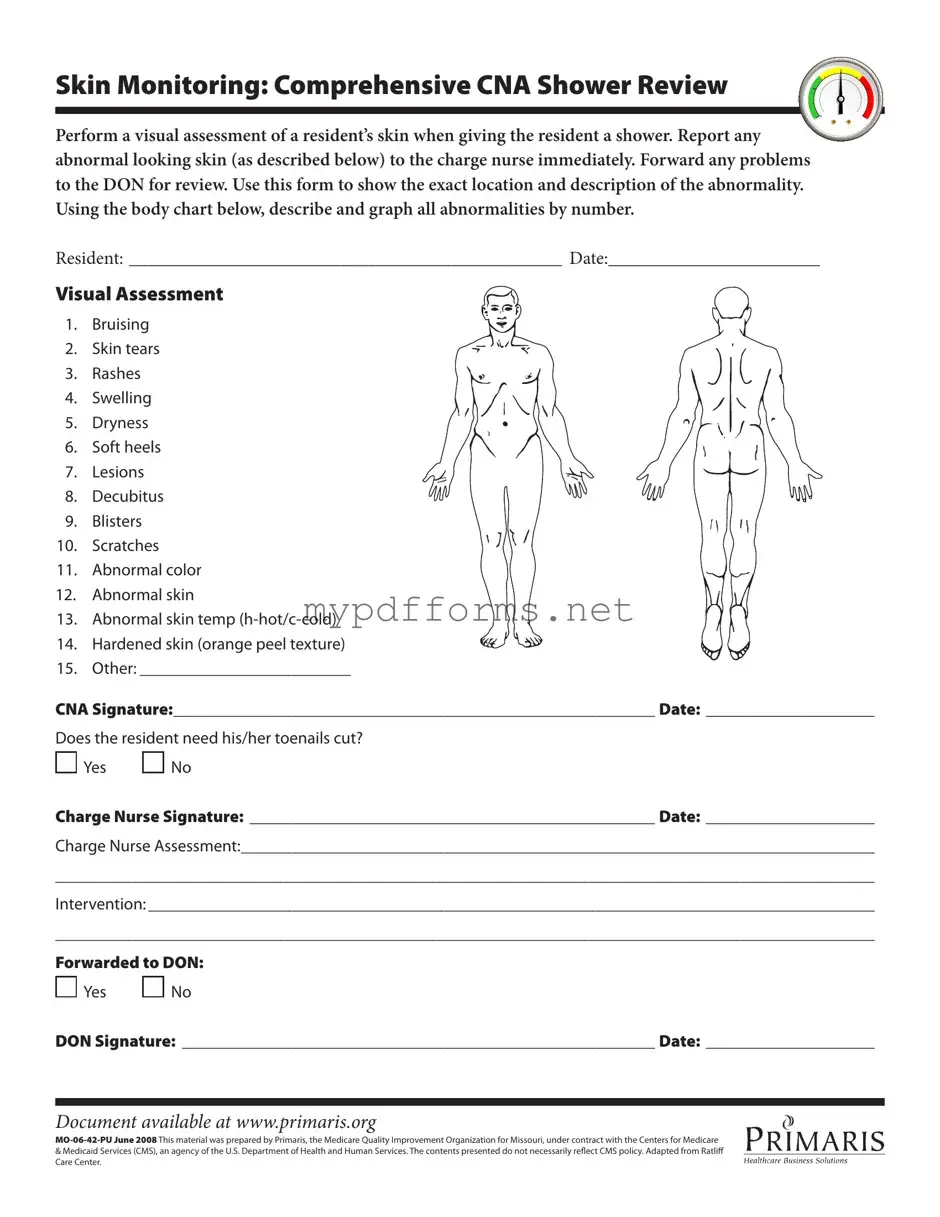
When caring for residents in a healthcare setting, meticulous attention to skin health is paramount, and the CNA Shower Sheets form plays a critical role in this process. This essential document serves as a comprehensive tool for Certified Nursing Assistants (CNAs) to conduct thorough visual assessments of a resident's skin during showering. By documenting various skin conditions, such as bruising, rashes, and lesions, the form ensures that any abnormalities are reported to the charge nurse without delay. It includes a body chart that allows CNAs to pinpoint the exact location of any issues, promoting clear communication and effective follow-up care. The form also addresses whether the resident requires toenail trimming, further enhancing personal care. With designated spaces for CNA and charge nurse signatures, the CNA Shower Sheets form not only facilitates immediate intervention but also tracks the ongoing skin health of residents. By utilizing this form, healthcare professionals can uphold the highest standards of care and safeguard the well-being of those they serve.
When filling out the CNA Shower Sheets form, it’s essential to follow certain guidelines to ensure accurate and effective documentation. Here’s a list of things you should and shouldn’t do:
Kink Checkbox - Intrigued by hot waxing, merging pain with beauty rituals.
Hurt Feelings Report - Encourages individuals to share and laugh about their sensitive moments.
In order to effectively manage your health and financial decisions when you cannot speak for yourself, it's crucial to understand the benefits of a Durable Power of Attorney form. This legal document not only grants a designated individual the authority to make decisions on your behalf but also ensures that your preferences are honored. For more information on how to obtain and complete this vital form, visit Illinois Forms.
D1 Application Form Download - Check if you can read a car number plate from a specified distance.
Here are some key takeaways for filling out and using the CNA Shower Sheets form:
Completing the CNA Shower Sheets form is essential for documenting skin assessments during resident showers. Accurate entries ensure that any abnormalities are reported and addressed promptly. Follow these steps carefully to fill out the form correctly.
What is the purpose of the CNA Shower Sheets form?
The CNA Shower Sheets form is used to monitor the skin condition of residents during showers. It helps Certified Nursing Assistants (CNAs) document any abnormalities they observe on a resident's skin. This includes issues like bruising, rashes, or any unusual changes. The form ensures that the charge nurse and Director of Nursing (DON) are informed about any concerns for further assessment and intervention.
How should I fill out the form?
To fill out the form, start by entering the resident's name and the date at the top. As you conduct the visual assessment during the shower, note any skin abnormalities in the designated areas. Use the body chart to indicate the exact location and description of each issue. After completing the assessment, sign and date the form. If the resident needs toenail care, check "Yes" or "No." The charge nurse will also need to sign and date the form after their assessment.
What types of skin issues should I look for?
During the assessment, look for a variety of skin issues. Common problems include bruising, skin tears, rashes, swelling, and dryness. You should also check for soft heels, lesions, decubitus ulcers, blisters, scratches, and any abnormal skin color or temperature. If you notice any of these issues, it is important to document them accurately on the form.
What should I do if I find an abnormality?
If you find any abnormalities during the assessment, report them to the charge nurse immediately. The charge nurse will then assess the situation further. Make sure to document the findings on the form, including any necessary interventions. This information will be forwarded to the DON for review if needed.
Where can I access the CNA Shower Sheets form?
The CNA Shower Sheets form can be accessed online at www.primaris.org. It is important to have the most current version of the form to ensure proper documentation and compliance with health care standards.
The CNA Shower Sheets form is similar to the Incident Report form, which is commonly used in healthcare settings to document any unusual occurrences involving patients. Both documents require detailed descriptions of observed conditions, ensuring that any abnormalities are noted and reported to the appropriate personnel. The Incident Report focuses on events such as falls or medication errors, while the CNA Shower Sheets specifically monitor skin conditions during bathing. Both forms aim to promote patient safety and facilitate communication among staff members regarding patient care.
Another comparable document is the Patient Assessment form, which serves to evaluate a resident's overall health status. This form includes sections for vital signs, medical history, and current health issues. Like the CNA Shower Sheets, it emphasizes the importance of thorough observation and documentation. Both documents require healthcare professionals to record specific findings, enabling a comprehensive understanding of the patient’s condition and informing subsequent care decisions.
The Care Plan form is also similar, as it outlines the strategies and interventions tailored to meet a resident's needs. This document, like the CNA Shower Sheets, requires input from various healthcare providers to ensure a holistic approach to care. While the Care Plan focuses on long-term goals and interventions, the CNA Shower Sheets provide immediate observations that can influence daily care practices, thereby enhancing the overall quality of care.
Similarly, the Skin Assessment form serves to monitor skin integrity over time. This document often includes a checklist of skin conditions and a section for documenting changes. The CNA Shower Sheets share this focus on skin health, emphasizing the importance of regular assessments during bathing. Both forms aim to identify potential issues early, allowing for timely interventions to prevent further complications.
The Medication Administration Record (MAR) is another document that bears similarities to the CNA Shower Sheets. While the MAR tracks medications administered to patients, it also requires staff to observe and document any side effects or reactions. Both forms prioritize accurate reporting and communication among healthcare providers, ensuring that any changes in a resident’s condition are promptly addressed.
In addition, the Daily Progress Notes are akin to the CNA Shower Sheets in that they record observations and updates on a resident’s condition. These notes provide a comprehensive account of a patient’s status throughout the day, including any changes in skin condition or other health indicators. Both documents serve as vital communication tools that help maintain continuity of care among staff members.
The Resident Care Log is another similar document, focusing on daily interactions and care provided to residents. This log captures various aspects of care, including personal hygiene and skin assessments. The CNA Shower Sheets specifically target skin monitoring during showers, while the Resident Care Log encompasses a broader range of daily activities, yet both emphasize the importance of documentation for effective patient care.
To effectively handle property transfers in Pennsylvania, understanding the Quitclaim Deed form is essential, as it allows for a seamless ownership change without title warranties. This document serves as a vital tool when ensuring clarity in such transactions, highlighting the importance of accurate documentation for all parties involved. For those interested in starting this process, it's helpful to utilize resources like quitclaimdocs.com/fillable-pennsylvania-quitclaim-deed/, which provide guidance on filling out the requisite forms correctly.
The Fall Risk Assessment form also shares a connection with the CNA Shower Sheets. Both documents are used to evaluate specific risks associated with patient care. While the Fall Risk Assessment identifies factors that may contribute to falls, the CNA Shower Sheets concentrate on skin integrity during bathing. Each document plays a crucial role in promoting patient safety by identifying potential issues that require intervention.
Lastly, the Vital Signs Record is comparable to the CNA Shower Sheets as both documents require regular monitoring of patient conditions. The Vital Signs Record focuses on physiological measurements, while the CNA Shower Sheets document skin conditions during bathing. Both forms are essential for tracking changes over time and ensuring that any emerging health concerns are addressed promptly.
The CNA Shower Sheets form serves as a crucial tool for documenting the skin assessment of residents during showering. In conjunction with this form, several other documents may be utilized to ensure comprehensive care and accurate record-keeping. Below is a list of related forms and documents often used alongside the CNA Shower Sheets.
Utilizing these documents in conjunction with the CNA Shower Sheets enhances the quality of care provided to residents. Each form plays a distinct role in ensuring that all aspects of a resident's health are monitored and addressed appropriately.
Below is a list of common misconceptions regarding the CNA Shower Sheets form, along with clarifications for each.
This form is designed to monitor a range of skin conditions, from minor issues like dryness to more serious concerns such as bruising and lesions.
CNA staff are responsible for performing the visual assessments and must report any abnormalities to the charge nurse immediately.
Using the CNA Shower Sheets form is a mandated procedure to ensure thorough skin monitoring for all residents during showers.
The body chart is a crucial part of the form, as it allows CNAs to accurately describe and graph the location of any skin abnormalities.
While the primary focus is on skin conditions, the form also includes a section for assessing the need for toenail care, which is an important aspect of overall hygiene.
The completed form must be forwarded to the Director of Nursing (DON) for further review and intervention, ensuring a comprehensive approach to resident care.
While all abnormalities should be reported, the appropriate intervention may vary based on the assessment by the charge nurse or DON.
A CNA signature is required to confirm that the assessment was completed, ensuring accountability in the documentation process.
The CNA Shower Sheets form is applicable to all residents receiving care, regardless of their specific health conditions.
While the form may have been adapted from previous versions, it is regularly updated to reflect best practices in resident care and skin monitoring.