Get Medication Administration Record Sheet Form in PDF
Get Medication Administration Record Sheet Form in PDF
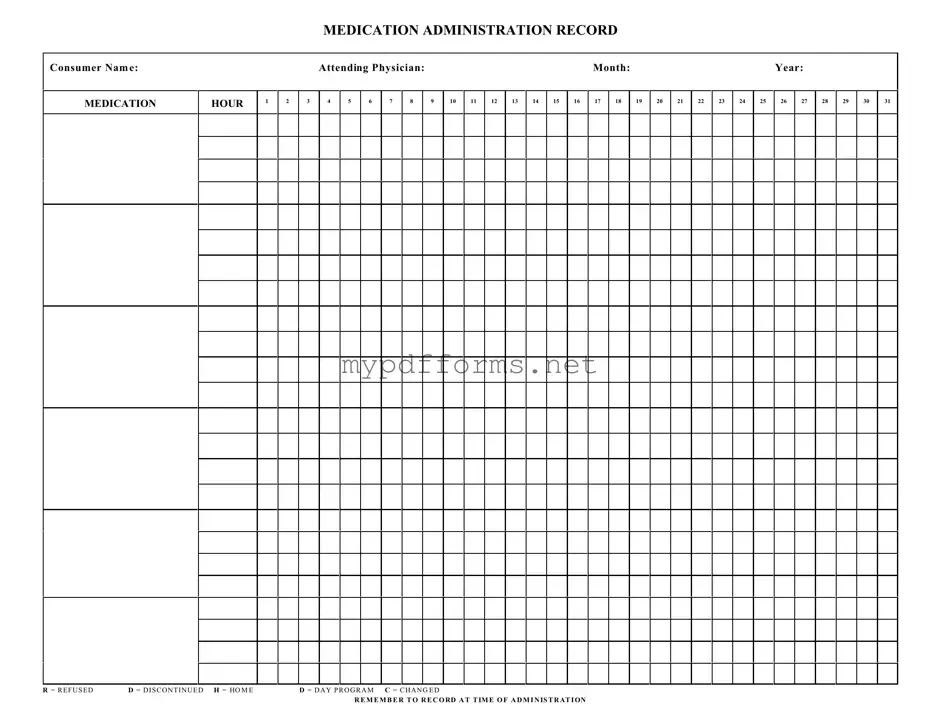
The Medication Administration Record Sheet (MARS) is an essential tool used in healthcare settings to ensure accurate tracking of medication administration for individuals receiving care. This form includes vital information such as the consumer's name, the attending physician, and the specific month and year for record-keeping. Each hour of the day is represented, allowing caregivers to document when medications are given. Additionally, the form features a series of codes to indicate various situations, such as when a medication is refused, discontinued, or changed. It emphasizes the importance of recording the time of administration, ensuring that all healthcare providers are informed of the medication schedule. By maintaining clear and organized records, the MARS plays a crucial role in promoting safe and effective medication management, ultimately supporting the health and well-being of consumers.
When filling out the Medication Administration Record Sheet form, it's important to follow certain guidelines to ensure accuracy and compliance. Here are five things you should and shouldn't do:
By following these tips, you can help ensure that the Medication Administration Record is completed correctly and effectively.
Cg 20 10 07 04 - This form allows for enhanced coverage, but careful attention to details is crucial.
For anyone looking to buy or sell a motorcycle in Georgia, it is important to utilize the Georgia Motorcycle Bill of Sale to document the transaction accurately. This legal form not only records the essential details of the motorcycle, such as its make, model, and Vehicle Identification Number (VIN), but also provides necessary proof of ownership transfer. To ensure a seamless transaction and protect your rights as a buyer or seller, you can find the form at https://motorcyclebillofsale.com/free-georgia-motorcycle-bill-of-sale/.
Bf Application - Seeking a fun-loving partner with a positive outlook.
When using the Medication Administration Record (MAR) Sheet, it’s important to keep a few key points in mind to ensure accurate and effective medication management.
Completing the Medication Administration Record Sheet is essential for maintaining accurate medication records for individuals. This form tracks medication administration, ensuring that each dose is documented correctly. Below are the steps to fill out the form effectively.
The Medication Administration Record Sheet is a vital tool used to track the administration of medications to consumers. It helps ensure that medications are given at the correct times and in the correct dosages. This form serves as a record for healthcare providers, ensuring accountability and continuity of care.
To complete the Medication Administration Record Sheet, start by entering the consumer's name, the attending physician's name, and the month and year at the top of the form. Next, use the grid provided to indicate the hours when medications are administered. For each medication, mark the appropriate box corresponding to the hour of administration. Use codes such as "R" for refused, "D" for discontinued, "H" for home, "D" for day program, and "C" for changed.
If a consumer refuses medication, it is essential to document this on the Medication Administration Record Sheet. Mark the box with an "R" at the corresponding hour of administration. Additionally, note the reason for refusal in the consumer's medical record to ensure that healthcare providers are aware of the situation and can address any concerns.
In cases where a medication is discontinued, mark the box with a "D" at the appropriate hour. It is also important to update the consumer's medical records to reflect this change. This helps maintain accurate medication history and ensures that all healthcare providers are informed about the current treatment plan.
Recording the time of administration is crucial for several reasons. It helps ensure that medications are taken as prescribed, which is essential for their effectiveness. Additionally, accurate timing can help identify potential issues, such as missed doses or adverse reactions. This information is vital for the healthcare team to provide the best care possible.
No, each Medication Administration Record Sheet is designed for individual consumers. This ensures that each consumer's medication regimen is accurately tracked and documented. Using a separate sheet for each consumer prevents confusion and maintains clear records for each person's unique needs.
The Medication Administration Record (MAR) is similar to the Patient Medication Profile. Both documents provide essential information about a patient's medications. The Patient Medication Profile lists all medications prescribed to a patient, including dosages and administration routes. This profile is often used by healthcare providers to ensure that they have a comprehensive view of a patient's medication regimen. The MAR, on the other hand, focuses on the actual administration of those medications, documenting when and how each medication is given. This helps to track adherence and monitor any potential issues in real-time.
Another document that shares similarities with the MAR is the Medication Reconciliation Form. This form is used to compare a patient's current medications with those prescribed during a healthcare transition, such as a hospital discharge. Like the MAR, the Medication Reconciliation Form aims to prevent medication errors and ensure continuity of care. Both documents require accurate and up-to-date information to be effective, and they play a crucial role in patient safety by identifying discrepancies in medication regimens.
The Illinois Application for Firearm Control Card is a critical document for those seeking to carry firearms professionally, ensuring that applicants meet necessary criteria such as age and background checks. To facilitate the process effectively, it is essential to utilize the appropriate resources for obtaining this form, including Illinois Forms, which provides guidance on completing the application accurately. By following the correct procedures, individuals can ensure compliance with state regulations while pursuing their licensure to carry firearms in their respective professions.
The Treatment Administration Record (TAR) is another document akin to the MAR. While the MAR specifically focuses on medications, the TAR encompasses a broader range of treatments, including therapies and interventions. Both documents serve to track the administration of prescribed treatments and ensure that patients receive their care as intended. The TAR may also include notes on the patient's response to treatment, which can be valuable for ongoing care decisions.
The Care Plan is also similar to the MAR in that it outlines the specific interventions and medications a patient requires. The Care Plan is a comprehensive document that details the overall strategy for a patient's care, including goals and expected outcomes. In contrast, the MAR is more focused on the execution of those plans, recording the actual administration of medications. Both documents work together to ensure that healthcare providers are aligned in their approach to patient care.
The Incident Report shares some similarities with the MAR in terms of documentation. While the MAR tracks medication administration, the Incident Report records any adverse events or errors related to medication use. Both documents are crucial for maintaining patient safety and quality of care. They provide a mechanism for healthcare providers to learn from errors and improve practices, although they serve different purposes in the overall care process.
Lastly, the Nursing Notes can be compared to the MAR. Nursing Notes document a patient's condition and any care provided, including medication administration. While the MAR is specifically focused on medications and their administration, Nursing Notes provide a broader context of the patient's health status and care interventions. Together, these documents create a comprehensive picture of the patient's care, allowing healthcare providers to make informed decisions.
The Medication Administration Record Sheet is a crucial document used to track the administration of medications to individuals in various care settings. However, it is often accompanied by other important forms and documents that help ensure proper medication management and compliance with healthcare regulations. Below is a list of related documents that are commonly utilized alongside the Medication Administration Record Sheet.
These documents collectively contribute to a more effective and safe medication administration process. Utilizing them in conjunction with the Medication Administration Record Sheet helps healthcare providers maintain high standards of care and compliance with regulations.
Misconceptions about the Medication Administration Record (MAR) Sheet can lead to confusion and errors in medication management. Here are ten common misunderstandings:
Understanding these misconceptions can enhance the effectiveness of medication administration and improve patient safety. Proper use of the MAR Sheet is a shared responsibility that requires diligence and attention to detail.